Shoulder ROM using a goniometer has been shown to have good reliability1 and poor reliability2 with up to 25° of measurement error. There are studies to show that use of Smartphone for measuring shoulder ROM to also have acceptable reliability3. I have however personally found both goniometer and Smartphones cumbersome.
Here are 4 easy and reliable (no study yet) shoulder ROM outcome measures that I personally use clinically.
Outcome measure #1: Shoulder Medial Rotation / Hand Behind Back (HBB)
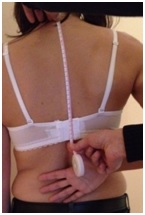
You may use a standard measuring tape and simply measure the distance from the most prominent spinous process at the cervico-thoracic junction (C7 or T1) to the tip of the thumb. The C7 is the most prominent spinous process in 75% of people and T1 is most prominent in 25% of people. The fact is that it doesn’t matter which spinous process is used as long as it is the same (most prominent) one used for both left and right shoulder and in between sessions.
I use this outcome measure on all my patients who report of pain and limitation with HBB such as those with impingement syndrome and adhesive capsulitis.
Outcome measure #2: Shoulder Lateral Rotation @ 0 abduction
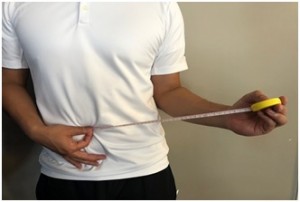
You may use a standard measuring tape and simply measure the distance between the umbilicus and the hand as the measuring tape is pulled away. Just make sure that the elbow is consistently flexed to 90° and is kept tightly by their side. The forearm is in neutral pronation supination.
I use this outcome measure on all my patients with shoulder pain to rule out adhesive capsulitis. Atraumatic loss of the LR at 0° abduction is the strongest predictor of adhesive capsulitis5.
Outcome measure #3: Wall Reach-up Test

You may use a stick on wall measuring tape (part of the STARmat package) and simply measure the distance reached. Just make sure the feet are facing the wall and that the toes are touching the wall.
I use this outcome measure on all my patients who have a loss of shoulder elevation for any reason such as post-op, pos-dislocation or adhesive capsulitis.
Measurements are usually accurate to the nearest 1-2 cm. Patients can turn this outcome measure into a motivating home exercise program on a wall or a door fame at home.
Outcome measure #4: Active Reach-up Test

You may use a standard measuring tape and simply measure the distance between the umbilicus and the hand as it is raised overhead.
I use this outcome measure on all my patients who have a loss of shoulder elevation for any reason such as post-op or adhesive capsulitis.
Patients simply love the Active Reach-up test and find it a motivating outcome measure. With each session, they attempt to beat their previous score.
- Mullaney MJ1, McHugh MP, Johnson CP, Tyler TF. Reliability of shoulder range of motion comparing a goniometer to a digital level. Physiother Theory Pract. 2010 Jul;26(5):327-33.
- Hayes K1, Walton JR, Szomor ZR, Murrell GA. Reliability of five methods for assessing shoulder range of motion. Aust J Physiother. 2001;47(4):289-94.
- Shin SH1, Ro du H, Lee OS, Oh JH, Kim SH. Within-day reliability of shoulder range of motion measurement with a smartphone. Man Ther. 2012 Aug;17(4):298-304.
- Wolf EM, Cox WK. The external rotation test in the diagnosis of adhesive capsulitis. Orthopedics. 2010 May 12;33(5).