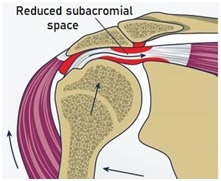
In 1983, Dr. Charles Neer, the developer of acromioplasty described impingement as “the compression of the bursal side of the rotator cuff (RC) beneath the anterior acromion”. It is at that time when the diagnosis of RC impingement syndrome was popularized. In the 80’s and 90’s, the surgery became the primary treatment for this hypothesized condition.
In case you need a refresher, you can view this one minute subacromial decompression surgery video to see what is often done.
Physiotherapy was thought of as something to do post-op but a waste of time when someone presented with “real impingement”. After all, how could any physiotherapy treatment increase the space underneath the acromion? Obviously a surgical procedure was necessary to remove or partially shave the acromion and remove the coraco-acromial ligament to increase the subacromial space.
Fast-forward to 2020 and it turns we were mostly inaccurate. After decades of placebo controlled studies, the latest systematic review shows that…
“There was high certainty evidence of no additional benefit of subacromial decompression surgery over placebo surgery in reducing pain at 1 year following surgery.” – Lähdeoja et al 2020
After decades of diagnosing and explaining RC impingement to hundreds of my patients, I am happy to say that I am no longer offering that diagnosis or explanation to any of my patients with shoulder pain.
I now offer them the diagnosis, “Rotator Cuff Sensitivity” (RCS). I know it’s not a term that is popular yet, but I am hoping that it will catch on. RCS is certainly less threatening than torn, pinched, inflamed, or impinged. In my humble opinion using the term RCS reduces the threat value of their condition and emphasizes that the goal is to desensitize the shoulder versus “fix” the shoulder.

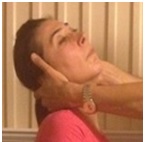
Do me favour right now, look up and fully extend your neck. Did you have pain shooting down your arm? Hopefully not! However you must appreciate that when you extended your neck, you technically “pinched” your C6 nerve roots within the intervertebral foramen. The reason you hopefully did not have pain shooting down into your arms was that your C6 nerve roots happen to not be sensitive. If your C6 nerve root was sensitized you would have undoubtedly had pain peripherlize down your arm, especially if you combined the extension with rotation.
We can safely conclude that nerve root “impingement” is not the issue as we all technically “impinge” our nerve roots when we extend and rotate; it is nerve root sensitivity that is the issue.
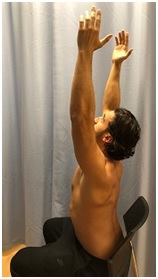
Now let’s do another practical test. Lift both your arms high over your head. Guess what? You just “pinched” all your subacromial structures and hopefully you do not experience pain. The reason some may experience pain with arm elevation may not be because of “impingement” (as we all experience that), but because of underlying RC sensitivity. Perhaps that is why the latest 2020 systematic review concludes…
“Subacromial decompression surgery provided no important benefit compared with placebo surgery or exercise therapy, and probably carries a small risk of serious harms.” – Lähdeoja et al 2020